You will need to be accompanied by car after the laser procedure.
Eye drops should be started as soon as you return home.
After LASIK surgery:
The hulls should be kept for 7 nights.
A sensation of grains of sand is common, with watery eyes.
Above all, don't hesitate to keep your eyes well hydrated with prescribed artificial tears (plenty of them, even 6 to 10 times a day if it makes you feel better).
Visual autonomy returns the next day.
Healing continues for the first month.
After a PRK operation :
A soft lens (conventional, without correction) is fitted after the operation. The aim is to improve healing and prevent excessive eye pain (bandage effect). This lens should be removed between the 3rd and 4th day after the operation.
Intense pain and photophobia are common in the first 2 days.
Painkillers are prescribed and must be taken immediately to help control the discomfort and pain.
Allow for 3 to 5 daysof social downtime (no computer use or driving).
Visual autonomy is slower than with LASIK, taking 5 to 7 days.
Healing continues for the first 3 months.
Note: At 3 months post-laser, neither technique (LASIK or PRK) has shown superiority in visual outcomes.
Cataracts correspond to the opacification of the crystalline lens (a normally translucent, high-power lens located inside the eye). Every year, 570,000 people are operated on in France. Surgery is the only way to improve vision altered by cataract.
There are no alternatives to cataract surgery.
Because neither eye drops nor lasers can cure an established cataract. In very advanced cases, cataract can cause blindness.
Worldwide, it is the leading cause of blindness due to the impossibility of large-scale treatment in third world countries. Tens of millions of people are waiting to be operated on, but unfortunately, due to a lack of human and financial resources, many of them will no longer be able to see because of their cataracts. For this reason, many humanitarian trips are organised, particularly to Africa.
Intervention is defined when the opacification of the lens is sufficiently significant, vision deteriorates slowly, often in distance vision with sometimes paradoxically a transient improvement in near vision without glasses.
The degree of discomfort is not the same for everyone. The decision to undergo an operation is therefore the result of a joint agreement between the ophthalmologist and the patient. Without surgery, the cataract will become denser and vision worse, and this may eventually affect fundus examination. Long-term cataract surgery has a current success rate of over 99.5%.
The surgery:
The procedure is usually performed under local anaesthetic using powerful anaesthetic drops.
Once the eye has been anaesthetised, a micro incision (approximately 2.2 mm) is made at the extreme periphery of the cornea. Then, using a ultrasound probe, the nucleus of the crystalline lens is destructured without damaging the capsule separating it from the posterior part of the eye (this is known as ‘phako-emulsification’). The nucleus of the crystalline lens is then removed to be replaced by a flexible implant. This is inserted folded, then unfolded where the crystalline lens used to be. There are several types of implant.
Currently, the femtosecond laser is used in cataract surgery.
It enables a precise incision to be made, the rhexis, a circular ring around the anterior capsule, to be cut and the nucleus to be cut. The result is greater precision and the use of less ultrasound. Its value is still debated.
In around 1 in 3 cases, a secondary cataract develops, corresponding to an opacification of the posterior capsule (left in deliberately during the operation in order to hold the implant in place). If the patient is bothered by a drop in visual acuity or a sensation of haze, this secondary cataract is treated by laser.
The treatment is carried out in consultation after instillation of drops to dilate the pupil. It is simple, safe, fast (usually less than 10 seconds) and painless.
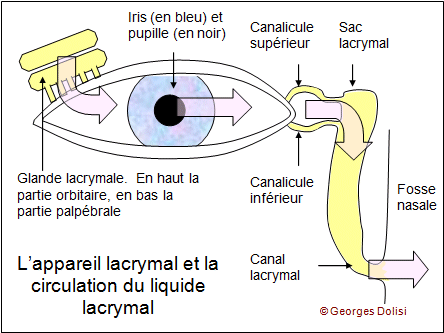
Dacryocystitis is an inflammation, usually of infectious origin, of a lacrimal sac. Dacryocystitis manifests itself by a typical continuous tearing, similar to that experienced during a cold. It occurs mainly at the extreme ages of life: in newborns and people over 70 years of age. In the elderly, dacryocystitis is linked to a narrowing of the lacrimal ducts. The reduced abundance of tears leads to an increased risk of infection.
In the early stages of the infection, treatment will consist of antibiotic therapy combined with local application of antiseptic eye drops.
When the infection is more advanced, an abscess of the lacrimal sac may occur, and a red and painful swelling may appear at the corner of the eyelid. In this case, the disease requires brief hospitalization.
After numerous recurrences and depending on the patient's discomfort, a dacryocysto-rhinostomy may be performed.
External dacryocysto-rhinostomy is the treatment of obstructions located in the nasolacrimal duct. The procedure is also performed via the endonasal route with similar results and complications, except for the absence of scarring with this technique.
It consists of bypassing the obstacle by creating a stoma between the lacrimal sac and the external wall of the nasal cavity.
An anastomosis will be performed between the lacrimal sac and the nasal mucosa. This is a preferable procedure to a dacryocystectomy in cases of dacryocystitis because it will not cause the patient to have permanent watering. The procedure has a success rate of approximately 90% and eliminates all symptoms. However, it is more difficult and time-consuming than a dacryocystectomy and requires specific equipment and expertise.
The procedure involves removing a piece of the bony wall between the lacrimal sac and the middle meatus of the nose, then suturing the mucosa of the sac to the nasal mucosa of the middle meatus.
Xanthélasma is a common condition that causes aesthetic discomfort and does not decrease with age. It is a xanthome plan palpébral (an infiltrate of histiocytic or macrophage cells filled with lipids – esterified cholesterol) that forms a yellowish plaque which gradually extends and darkens over the years on the upper or lower eyelid.
The best treatment is surgical, performed by an ophthalmologist, or if the lesions are small, they can be removed with a laser by a dermatologist.
However, recurrences are common, around 50%, which necessitates further treatments.
The major issue is the risk of ectropion due to skin retraction after multiple treatments.
Ectropion refers to the outward turning of the eyelid's free edge ("eversion" of the eyelid), causing a loss of contact between the eye and the eyelid.
The causes can be diverse:
Ectropion involutif: occurring due to tissue changes (progressive laxity) related to aging.
Ectropion paralytique: secondary to facial paralysis, related to certain myopathies, etc.
Cicatricial entropion: following burns or certain diseases (such as trachoma, etc.).
The treatment for ectropion is surgical and involves the correct repositioning of the eyelid tissues.
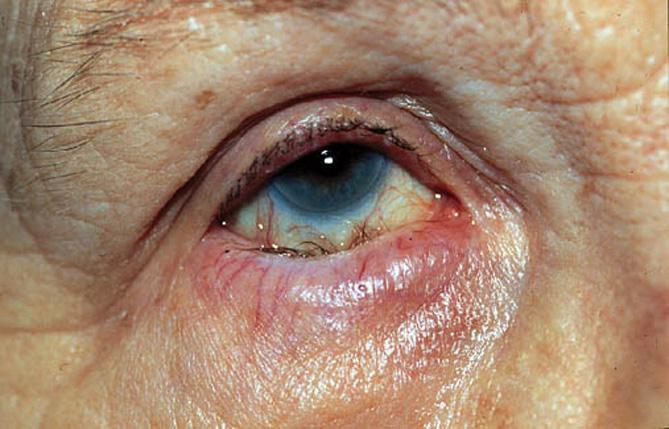
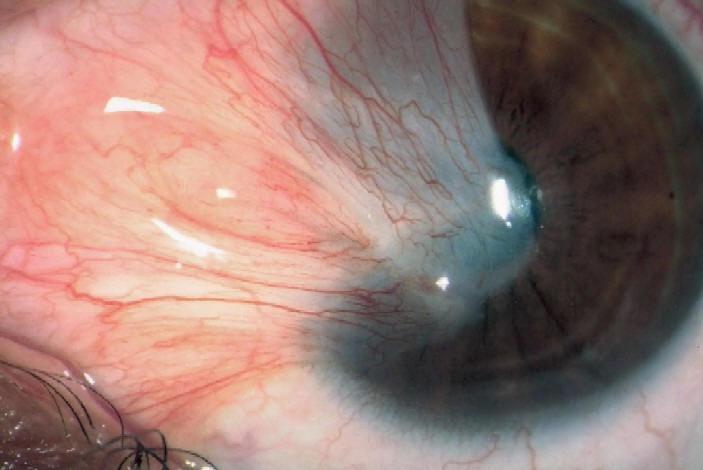
Pterygium is a benign tumor of conjunctival origin invading the cornea. It is most often located in the "white" of the eye in the inner angle of the eyelids (the canthus), on the nasal side. This conjunctivo-elastic tumor most often takes the shape of a triangle compared to a "wing" (Greek etymology of the term pterys).
Promoted by UV exposure and dry eyes.
Surgical treatment of pterygium has several objectives:
Maintain visual function threatened by progressive invasion of the corneal surface, restore the aesthetics of the eye, prevent recurrences, restore visual function in the event of invasion of the pupillary area.
Spontaneously, after a simple excision, recurrence occurs in a significant proportion of cases, varying according to the development of the lesion and the primary or secondary nature of the intervention.
It is important to carefully determine the time of the surgical indication because the more operations are performed, the greater the risk of recurrence.
This poses therapeutic problems, due to the exhaustion of the conjunctival capital available for autografting. It is therefore essential to implement the best possible preventive strategy from the first pterygium operation.
To avoid frequent recurrences, some methods are based on the destruction of conjunctival fibroblastic cells, application of mitomycin C or other antimetabolite agent (thiothepa), radiotherapy by beta irradiation with Strontium 90.
The majority of methods currently used include reconstruction of the excision area:
>par une autogreffe de conjonctive, excellente méthode et simple,
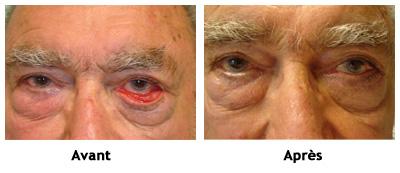
Ptosis refers to a drooping of the upper eyelid. It can be unilateral or bilateral, depending on whether it affects one eye or both, and is caused by a deficiency of the "levator" muscle of the upper eyelid.
Several factors can be the cause of ptosis:
In the case of aging, the eyelid muscle thins and may sag with age.
A neuromuscular disorder, ptosis can then be the first sign of a muscle disease; trauma, such as a blow to the eyebrow arch; or a congenital predisposition.
The main treatment is based on a simple surgical procedure. It involves "re-attaching" the upper eyelid to the muscle. Health insurance will not cover this procedure if the purpose is solely aesthetic.
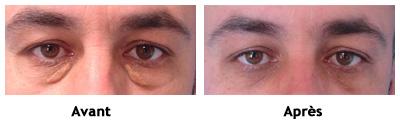
Very fine and delicate, blepharoplasty (correction of the lower and/or upper eyelids) provides great satisfaction by rejuvenating the eye contour.
Most often performed under local anesthesia with or without sedation, but sometimes upon request, under general anesthesia. The procedure lasts about one hour, and you can leave after one to two hours of rest or stay overnight.
The excess skin and fat pockets are removed through an incision in the natural fold, at the crease of the upper eyelid. The fat pockets of the lower eyelid can be removed through an incision beneath the lash line if there is excess skin. Otherwise, this can also be done without a scar via conjunctival approach. A bandage is optional for a few hours to avoid hematomas and bruising.
You may have traces of the procedure for 8 to 10 days, but activity is still possible with sunglasses with tinted lenses. It is a delicate and meticulous procedure, but it is light and has nothing to do with the ocular globe or vision.
Complications are exceptional.
An ectropion (outward turning of the lower eyelid) may occur if the technique is not properly performed. The eye contour will be rejuvenated, but a few years later, there may be the possibility of another procedure.