KLEX – Refractive Surgery by Lenticule Extraction
This technique is still under development, and we will only offer it to our patients once the manufacturers have made significant progress.
KLEX (Keratorefractive Lenticule EXtraction) is an advanced laser vision correction technique used to treat myopia (nearsightedness) and astigmatism, without creating a corneal flap. It is part of the same family as SMILE, SILK, CLEAR, and SmartSight.
🔹 Procedure Steps
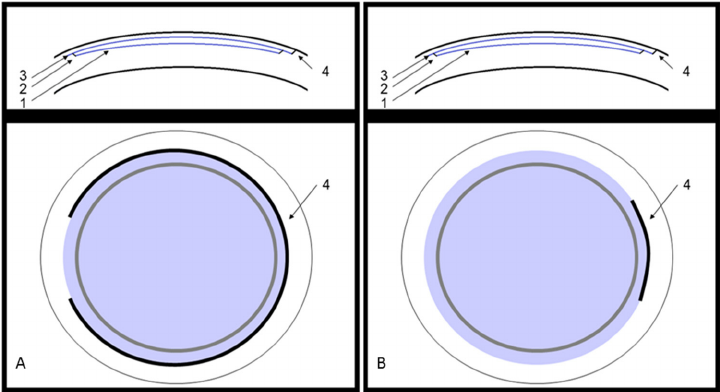
- The femtosecond laser creates a small lenticule within the cornea.
- The surgeon manually removes this lenticule, reshaping the cornea to correct the refractive error.
🔹 Platforms and Technologies
- Zeiss – SMILE (Visumax 500 or 800)
- Johnson & Johnson – SILK (Elita laser)
- Ziemer – CLEAR (Z8 laser)
- Schwind – SmartSight (Atos laser)
All these techniques share the same principle: a lenticule is created and manually extracted to reshape the cornea.
🔹 Technical and Clinical Considerations
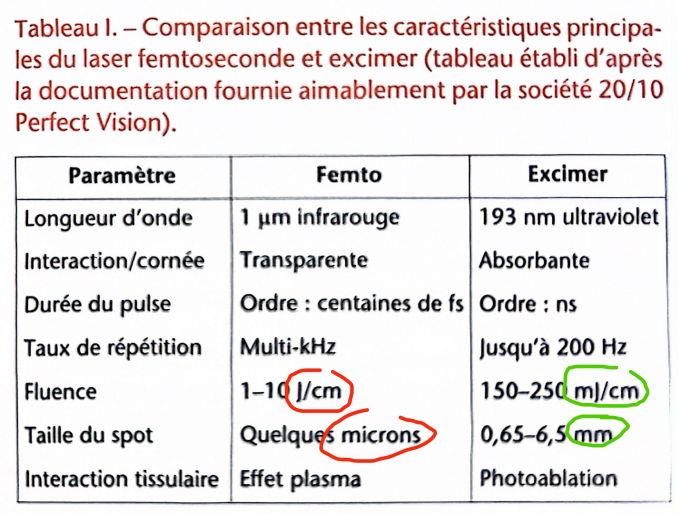
The KLEX technique does not use an excimer laser, making it less costly than LASIK. However, the excimer laser offers submicron precision and a smooth, continuous ablation, allowing for more accurate and extensive corrections.
The femtosecond laser, by contrast, uses 5–10 micron pulses in a dotted pattern, resulting in less refined tissue removal.
Despite being described as “minimally invasive,” KLEX is actually more manual than LASIK: the surgeon must dissect the lenticule with a spatula and remove it through a small side incision.
To prevent tearing, the lenticule edge must be at least 10 microns thick, leading to removal of ~15 microns of non-optical tissue for handling.
🔹 Advantages and Limitations
Theoretical advantages (less corneal cutting, better nerve preservation, reduced dryness) remain unproven.
Potential drawbacks include:
- manual centration (no automated eye tracker)
- meticulous dissection to avoid residual fragments or folds
- increased risk of decentration
🔹 Postoperative Recovery
Temporary blurred vision is common for several weeks or months due to mechanical dissection stress. Final results are comparable to LASIK, but without the typical “WOW effect” (clear vision the next day).
🔹 Biomechanical Aspects
Claims of better corneal stability than LASIK or PRK (especially for thin corneas) are theoretical and not confirmed by clinical studies.
A cornea that is unsafe for LASIK is also unsafe for SMILE or KLEX.
⚠️ Complications in SMILE and LASIK
Intraoperative (during surgery)
- Loss of suction
- Black spots
- Abrasions
- Epithelial incision tear
Specific to SMILE / KLEX:
- Difficult dissection (OBL – opaque bubble layer)
- Lenticule tear
- Lenticule remnants
- Cap perforation
- Incomplete lenticule extraction
Postoperative (after surgery)
- Corneal haze
- Irregular astigmatism
- Ectasia
- Interface infection
- Interface inflammation (keratitis)
- Loss of best-corrected visual acuity (BCVA)
- Blurred or “foggy” vision
- “Rainbow glare”
- Cap displacement or folds (specific to LASIK)